
Health and Well-being - Part 11 - More and Better Data
There are only two kinds of people in the world: Those who can extrapolate conclusions from incomplete data.

[NB: The Health and Well-being series of articles are reworked and updated from a similar series that first appeared on The Stoic Agilist. My goal for this series of articles is to serve as an example of how anyone might go about improving and sustaining their health and well-being.]
There are gaps in my health data. There always were and there always will be. But after working my way through the Early Medical program (twice) I have a much better understanding of where those gaps are and the relative importance for filling them. Some gaps I can’t change, like much of my family’s health history. It simply wasn’t recorded.
I focused first on filling out my cardiac health picture. It seemed to have the fewest gaps and the easiest access to tests that would fill in those gaps. There was also enough data at hand to suggest where to go next for information. The long running history of elevated cholesterol, ApoB, and elevated numbers of small and medium sized LDL particles run counter to the a calcium score of zero for someone my age. But the build up of calcium is usually a late stage arteriosclerosis symptom. I needed to know if a buildup of soft plaque in my arteries was occurring. After a somewhat arduous adventure arranging for a coronary CTA, the results were a score of zero (again) for the calcium scan portion of the test. As for soft plaque: “There is no CT evidence of hemodynamically significant coronary artery stenosis.” Translation: “My heart’s blood vessels are clear enough such that blood is flowing normally, and there’s no sign of serious narrowing that could lead heart problems.”
A conundrum.
After meeting with my cardiologist, the assessment was that it’s rare for someone my age to have a calcium score of zero and coronary arteries essentially clear of soft plaque while also having elevated levels of cholesterol and small/medium LDL particles. The condition is rare and suggests a genetic predisposition against heart disease. The recommendation was to check again in five years while continuing to monitor cholesterol levels.
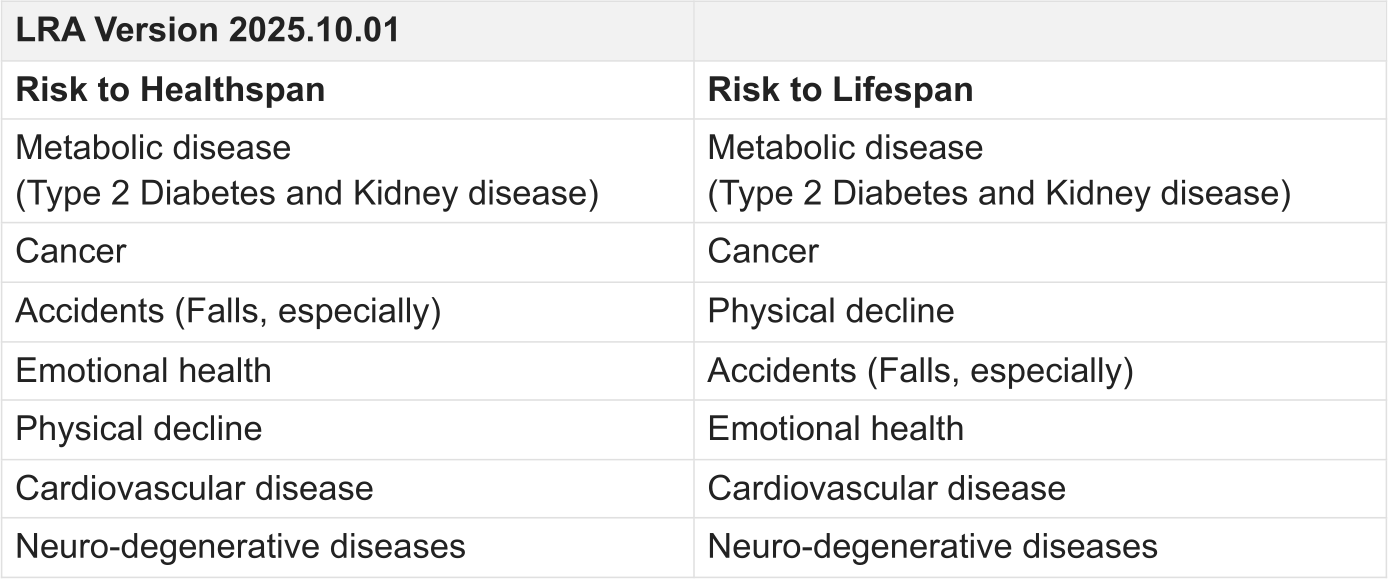
Hmmm. For someone who’s had to deal with the short end of the stick much more often then not, this is a welcome surprise. I’m still soaking in what this means exactly, but I’ll gratefully take the win. This shifted “Cardiovascular disease” down on the list of “Risks to Lifespan” for my Longevity Risk Assessment.
The plan is to continue researching the genetic angle. However, the results have also given me more confidence for pushing myself physically and consider a VO2 Max test at some point. My interest has also grown in exploring any possible connections between insulin resistance, elevated cholesterol, and free fatty acids/triglycerides.
Of Attia’s four horsemen of chronic disease, it looks like three of them are fading on the trail toward my marginal decade. I should add that I like Attia’s thinking around immune function as a fifth horseman, so I’ll put that one on the trail as well. But hot on my heels and gaining ground until very recently is metabolic disease.
The case of metabolic disease serves as a cautionary tale for over optimism based on incomplete data. I knew things weren’t going in my favor. What I didn’t fully appreciate is the systemic reach of metabolic disorders. The bigger picture became more focused as I continued to work out my specific insulin resistance phenotype based on DeFronzo’s1 “Ominous Octet.” After completing version 1 of my phenotype, I concluded:
“Given what I know at the moment, it appears that I’m dealing with early to mid systemic insulin resistance issues.”
What I know now is my assessment was optimistic. I’d already taken action to address the trend in A1c by electing a non-insulin pharmacological intervention. This had a clear effect on my A1c, sending it back into the pre-diabetic range after just two month. But I hadn’t fully appreciate the timing of the trend or its implications beyond “something is changing.” Reading further into DeFronzo’s work regarding the Ominous Octet, this caught my attention:
“Collectively, these eight players comprise the ominous octet and dictate that: 1) multiple drugs used in combination will be required to correct the multiple pathophysiological defects, 2) treatment should be based upon reversal of known pathogenic abnormalities and not simply on reducing the A1C, and 3) therapy must be started early to prevent/slow the progressive β-cell failure that already is well established in IGT [impaired glucose tolerance] subjects.”
...
“The resultant hyperglycemia and poor metabolic control may cause a further decline in insulin sensitivity, but it is the progressive β-cell failure that determines the rate of disease progression.”
I needed more and better data to assess where I was on the spectrum. The plan for acquiring a continuous glucose monitor (CGM) was moved up and, after another lengthy process that moved at the speed of paperwork, acquired a Dexcom G7 CGM about three months after initiating the pharmacological intervention. I wanted this monitor because it takes a glucose reading every 5 minutes.
After two weeks of monitoring it was clear I was in a state of poor metabolic control. I was sailing much closer to the rocks than I realized. After four weeks a couple of reliable patterns emerged: 1) it was very clear there are certain foods I absolutely must avoid and 2) while my blood glucose goes up after eating a meal - something that’s normal - it would often stay elevated for hours - something that’s not normal. While the pharmacological intervention was addressing insulin resistance in the liver and my modified exercise/strength training was designed to address muscle insulin resistance, the elevated levels of glucose for several hours seems to suggest - near as I can determine from reading the science - compromised pancreatic function. Either with α-cells, β-cells, or more likely both.

The Dexcom website tracks many useful metrics, but was missing a few that I wanted. So I modified the application I wrote for tracking health markers to collect additional data, correlate it with the CGM data, and ask different questions of the data.
I wanted to see how the mean and median glucose values were changing across successive 7 day periods. For the first 7 day period, the mean was 166 mg/dL and the median was 161 mg/dL. Three months later, after additional lifestyle changes (diet and exercise), the mean was 132 mg/dL and the median was 128 mg/dL. A clear shift in a positive direction. However, the distribution continues to skew a bit to the right showing that the high values are dominating. If course, the objective isn’t perfect alignment between the median and the mean. But the gap between the two can be used as an indicator - for my data - of how well I’m recovering from spikes. Over the course of three months the CGM shows a shift in this gap from 5 to 4 mg/dL. With more data and time, assuming continued improvement, I would expect this gap to narrow.
I wanted to correlate the continuous data to external events such as meals, drinks, activities, and sleep. I kept a daily journal of everything I ate or drank, activities (including sedentary ones such as coding or writing), and how well I slept. This gave me the insight I need to identify which foods caused spikes (carbohydrates in the form of sugar and flour) and which didn’t (protein.) Over time, I was also able to observe that average glucose levels became lower and lower during sleep - a good thing as it seemed my body was getting better at managing glucose. One puzzling result, which my doctor couldn’t explain and I haven’t yet found an answer for in the research, was that after drinking alcohol (red wine or scotch), my glucose level would go down. This happened repeatedly.
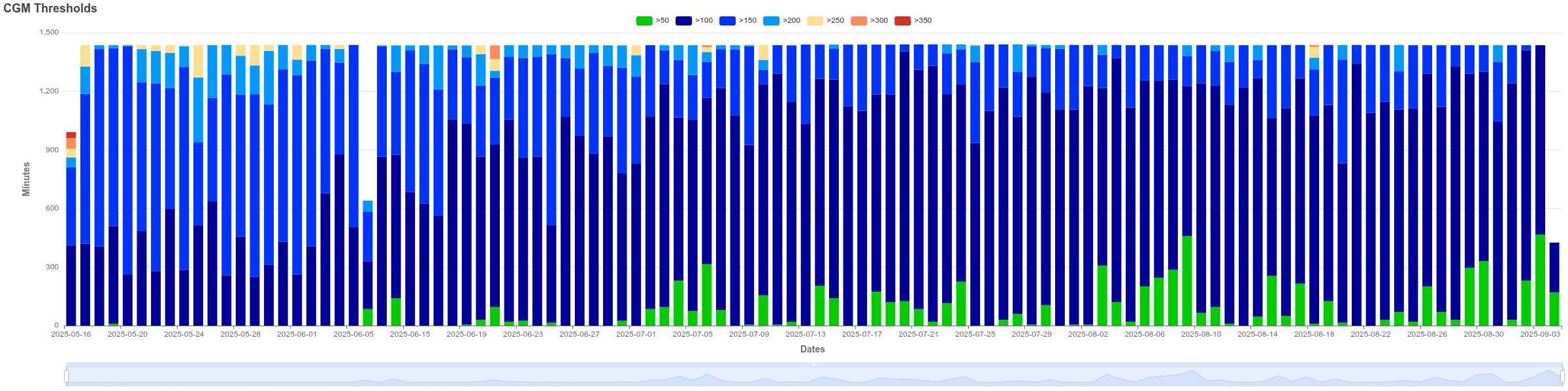
I wanted to know how much time I was spending in each of seven different value ranges. Here again, the news was good. Each slice in Figure 1 represents one day - 24 hours of data accumulated in 5 minute intervals. Over the course of three months, time spent in the high levels decreased and disappeared altogether. When exceptions occurred, I understood why they happened and even expected them (for example, celebrations where I ate what I wanted or travel where my choices were limited.) My target has been to spend at least a third of the time in the 50-100 mg/dL range while rarely going above 150 mg/dL. Just before discontinuing the CGM monitoring, it was clear I was approaching that goal.
This shift occurred over 3 months. That’s much longer than I would have expected, much less liked, and highlights several points:
The effort it takes to turn things like this around.
The importance of intervening as early as possible.
Collecting data that is specific to your phenotype.
Currently, I’m taking a break from the CGM and will resume just before the holidays. There are a couple of objectives for doing this. First, by removing the guardrails and gliding on my own for a while I’ll have a better sense of how I’ve adjusted to the needed lifestyle changes once I resume monitoring. When the monitors aren’t watching, am I staying on track with my goals? Secondly, monitoring all this health data is a royal pain in the butt. And it can get expensive. Absolutely necessary, to be sure, but I don’t want to do this for the rest of my life. I feel fortunate that I don’t have to and the plan is to keep it that way. Assuming I right this boat, the plan will shift to occasional monitoring of key indicators relevant to my phenotype.
Disclaimer
The author has Bachelor degrees in both biochemistry and cell biology but is not a licensed practitioner of medicine or psychotherapy and nothing presented on this website claims or should be construed to provide medical or psychotherapeutic advice. This series of articles is presented as a personal reflection by the author on work he’s done to improve his health and as such is relevant to the author and no one else. The author makes no recommendations as to any course of action the reader may chose to follow other than to encourage the reader to work closely with qualified health professionals when making healthcare decisions relevant to their personal lives.
← Health and Well-being - Part 10.2 - Resistance is Futile?
“Health and Well-being - Part 11 - More and Better Data” last updated on 2025.11.16.
I hope you will return regularly to The Remnant’s Way as I often update posts, particularly Ab Initio, and do not always publish to email posts that are meant to support or serve as reference to existing or future posts.
And please consider becoming a paid subscriber. Doing so supports my writing efforts and grants me the most precious of all resources - dedicated time for writing. And for that, I am deeply grateful. If you prefer, buy me a cup of coffee if there is an article here and there that you enjoyed or found valuable.
Image credit: Grok 4
Footnotes
DeFronzo, R. A. (2009). From the triumvirate to the ominous octet: A new paradigm for the treatment of type 2 diabetes mellitus. Diabetes, 58(4), 773–795. https://doi.org/10.2337/db09-9028