
Health and Well-being - Part 7 - Assessing Risks
"Risk is what's left over when you think you've thought of everything." - Carl Richards


[NB: The Health and Well-being series of articles are reworked and updated from a similar series that first appeared on The Stoic Agilist. My goal for this series of articles is to serve as an example of how anyone might go about improving and sustaining their health and well-being.]
The Early Medical program tasks participants with developing their Longevity Risk Assessment (LRA) - a process designed to help us determine our individual risks to healthspan and lifespan. In Dr. Attia's words, the LRA is about "charting our icebergs." That is, determining our health risks as framed with the Titanic metaphor. I, like Dr. Attia, love metaphors (Remember the captain of the Kōkai from Health and Well-being - Part 3 - Goals?) and the Titanic is a particularly good one for health. Most of us blissfully cruse along in what amounts to the foggy night of our health, trusting all is well and insulated by some version of "that won't happen to me" or "I'm too young for that." Until BANG. Iceberg. Our life crashes square into a life altering diagnosis, ripping a huge gash in our plans.
"How could I possibly have missed such a thing?" we ask. "Someone should have told me about that!" we yowl. We lash out, tilting at healthcare windmills and re-arranging the deck chairs while the situation grows worse. If we're lucky, the cold breeze of reason flowing off the iceberg chills our emotions and we acknowledge, "Yes, I had a hunch that was there. I should have checked." Then we get to work on making repairs if we can and changes in behavior because we must.
The LRA begins by considering some broad strokes data available to anyone who is interested, by evaluating statistical risks across various population sets. I added several sets of correlation data not considered in the Early Medical program. Figure 1 shows the percent distribution of the 10 leading causes of death, by sex in the United States (2021).
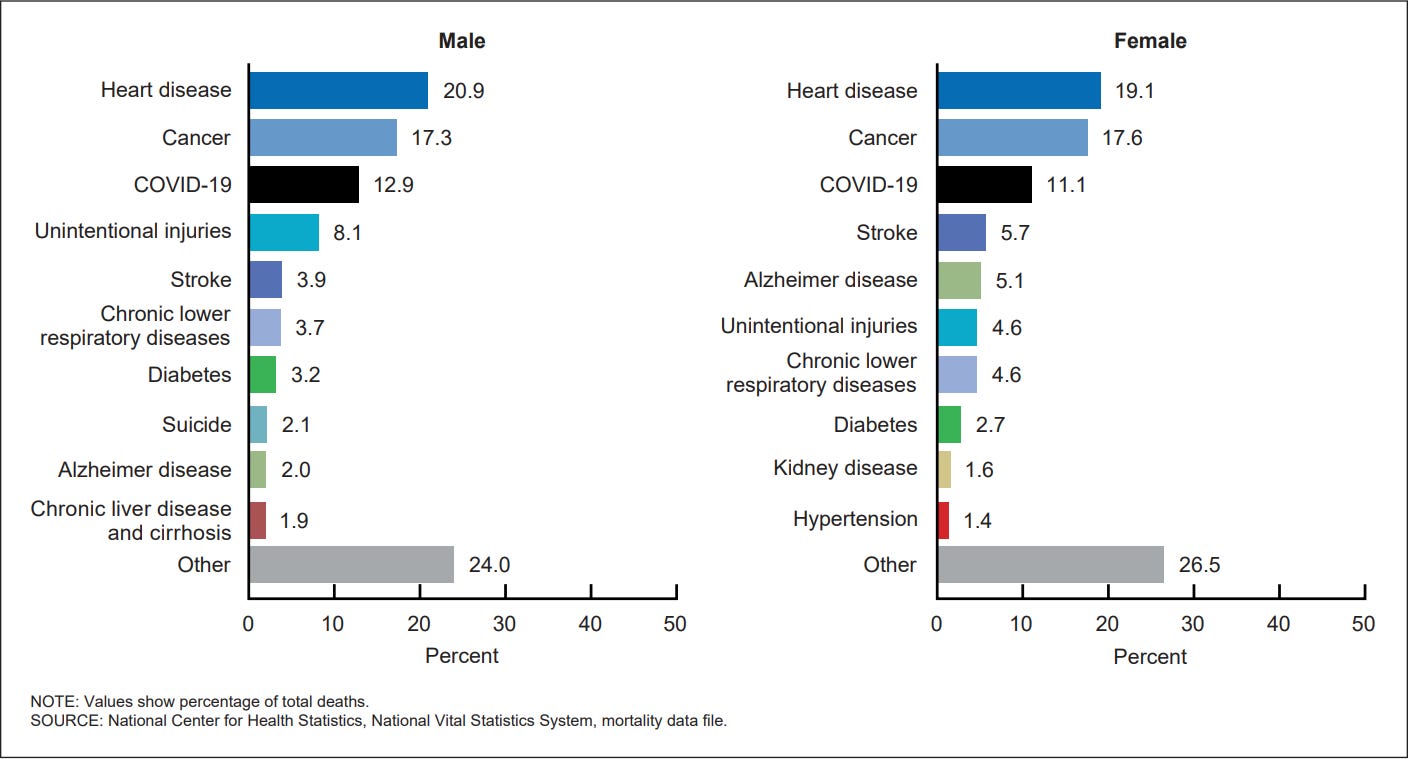
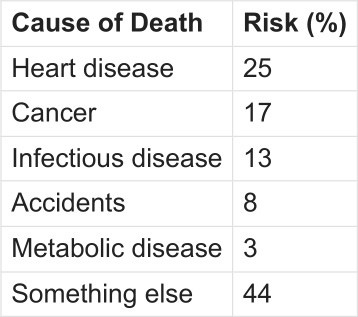
Since the leading cause of strokes is atherosclerosis, I rolled that risk into the heart disease numbers. Given my age, I considered COVID-19 in a more general case of "infectious diseases." To my knowledge, I've never had COVID. The few times I've been sick in the past five years tested negative for COVID. Perhaps the vaccinations worked as advertised. Diabetes I considered more broadly as "metabolic disease." "Chronic lower respiratory diseases" was shifted into "Other" because this category is most likely relevant to smokers and I don't smoke. My initial working set of the top statistical heath risks by virtue of living in the USA:
Your list will probably look different. Figure 2 shows the percent distribution of the 10 leading causes of death, by age group in the United States (2021).
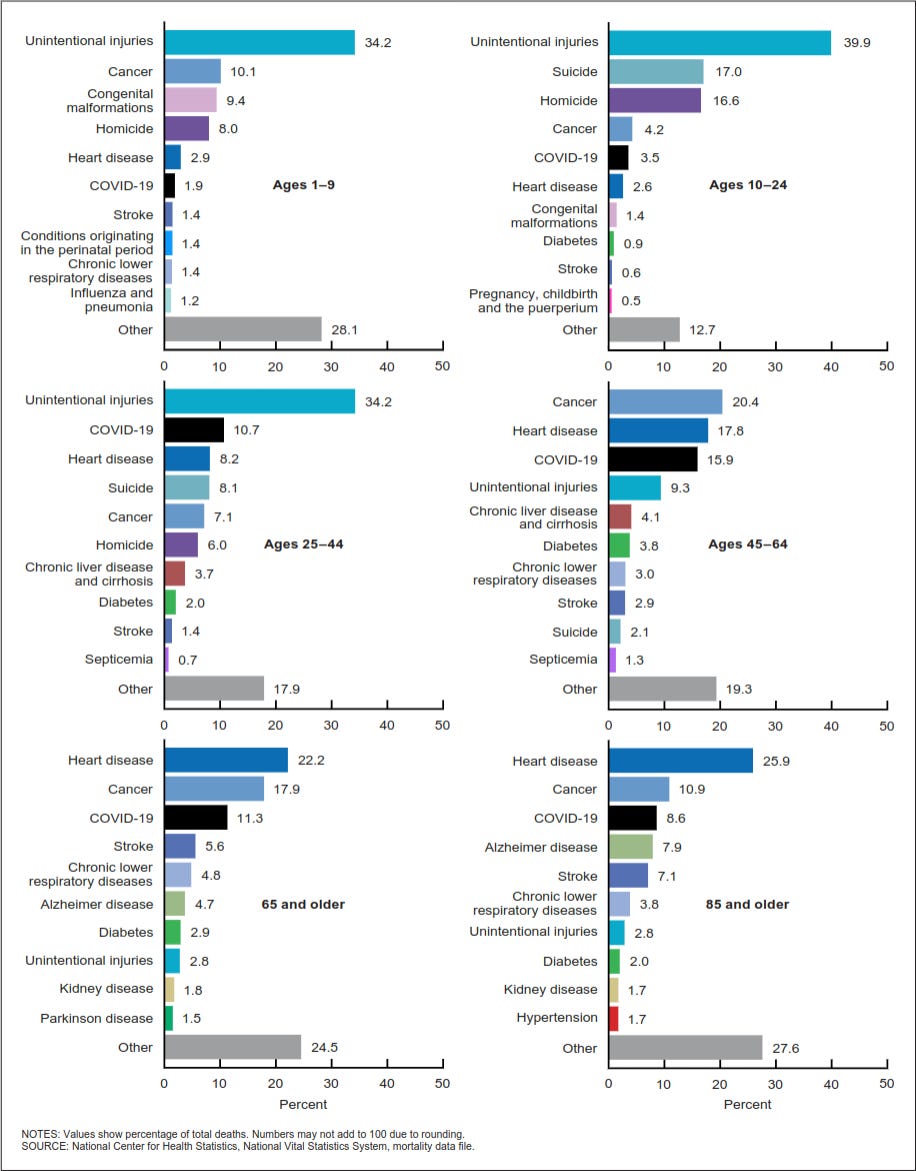
This picture alters my risk profile a little. I rolled kidney disease into metabolic disease since diabetes is the leading cause of kidney disease.
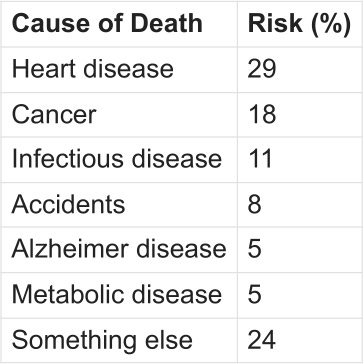
Again, your list will probably look different. Interesting that "Something else" has dropped by nearly fifty percent. The older we get the more clearly we can define what our death looks like. Figure 3 shows the life expectancy at age 65 for each state in the United States (2021).
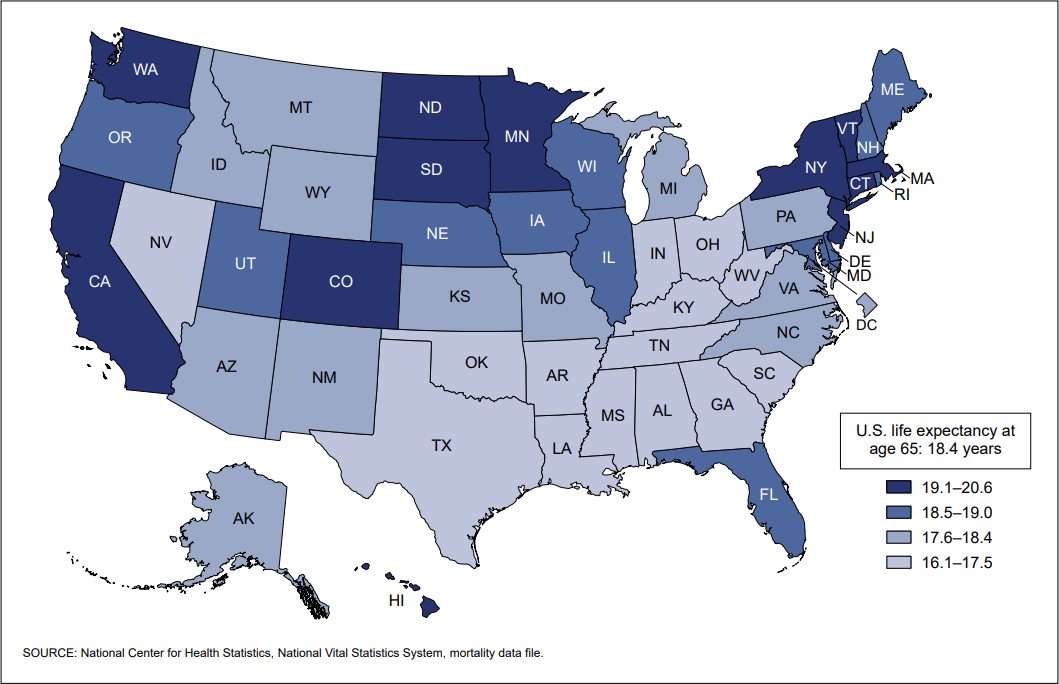
Hmm. Looks like, statistically, I get a little bit of a corollary bump for living in Colorado. Maybe reaching for a marginal decade between 75 and 85 years of age isn't so far fetched. Figure 4 shows the age-adjusted death rates by marital status for adults aged 25 and over in the United States (2010-2019).
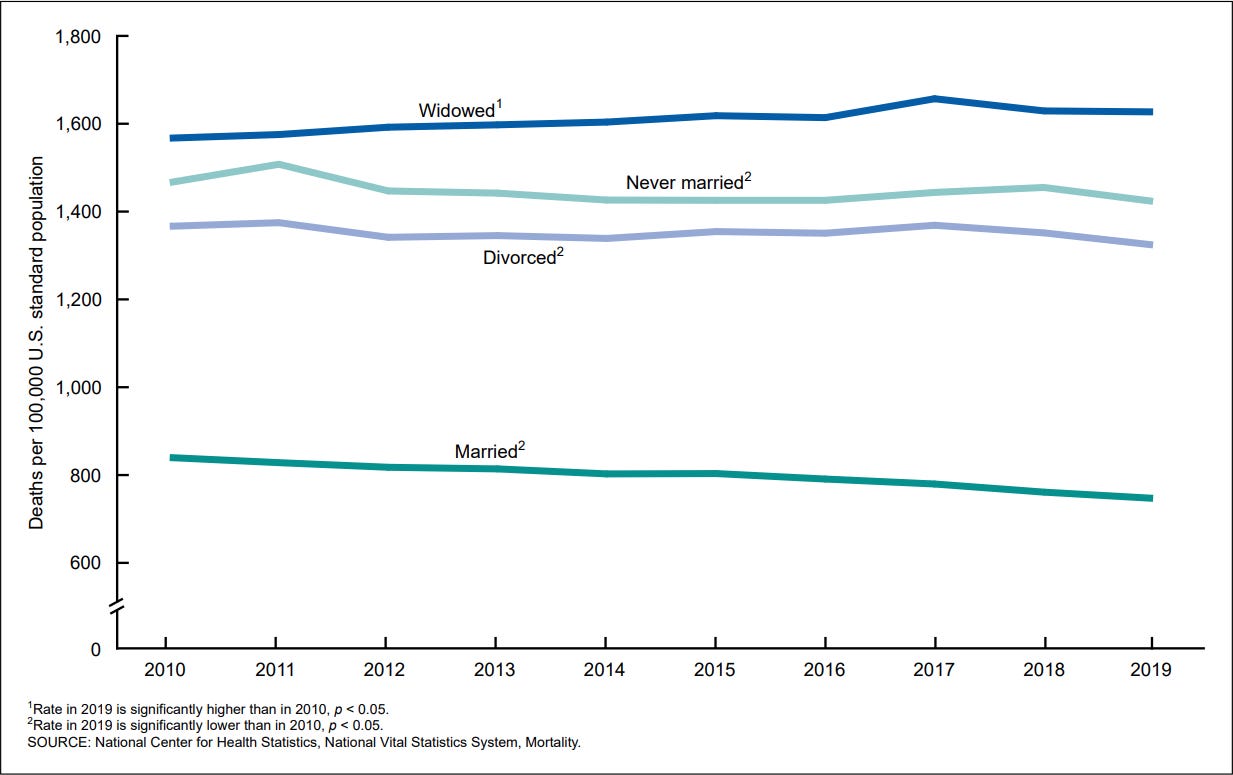
Extra bonus, I'm happily married. However, there was that 10 year cancer battle during my late 30's and early 40's after which I was widowed for about five years. While I consider my first marriage happy, it was also many times incredibly stressful. Undoubtedly, the stress from that 15 year stretch exacted some kind of toll. I've written before about the impact of these years on my diet and sleep. I've often wondered what else may have been adversely affected.
Figure 5 breaks out the age-adjusted death rates for adults aged 25 and over for the 10 leading causes of death by marital status in the Unites States (2019).
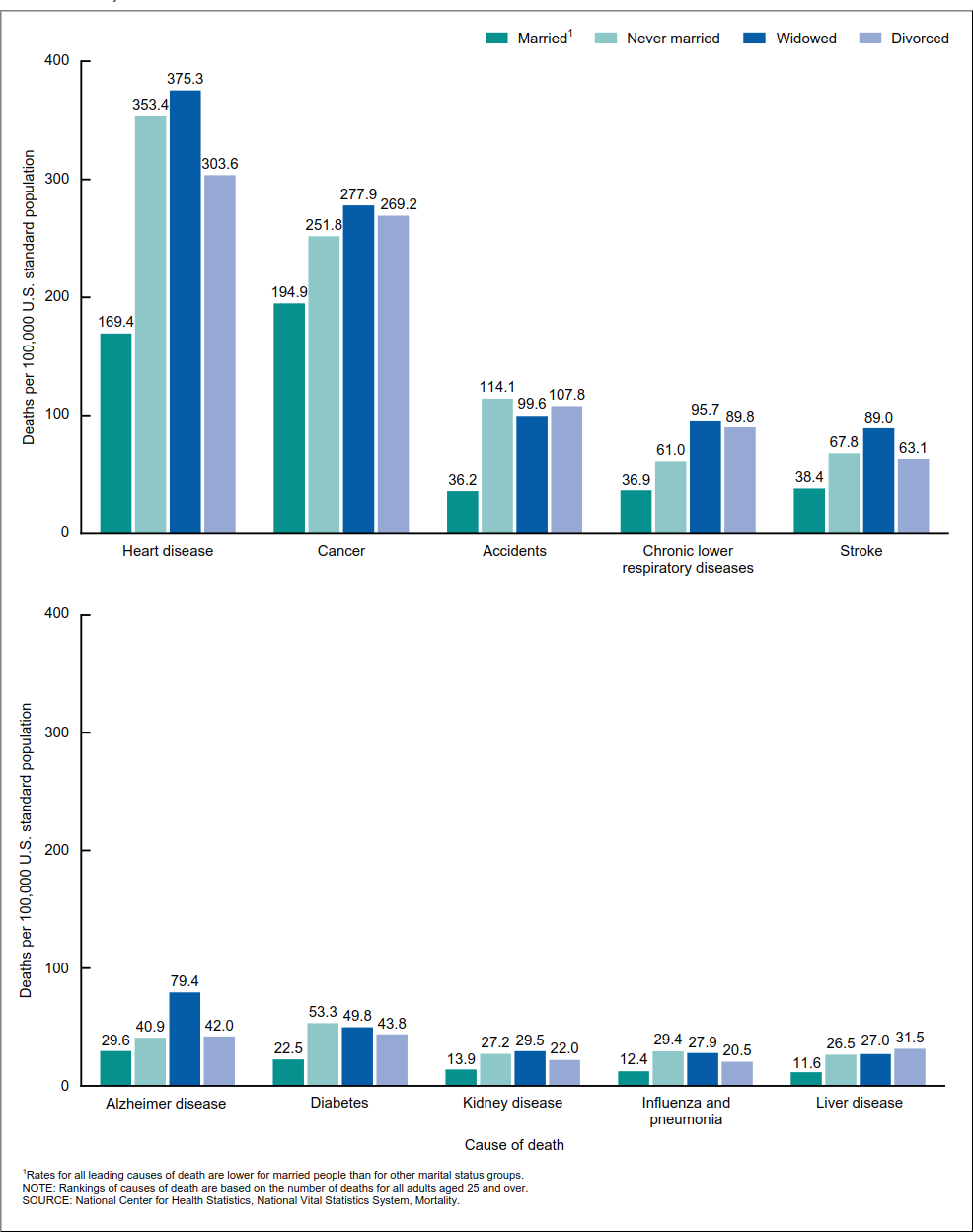
The data aren't broken out by sex, unfortunately, but I would guess that since men die younger and the status of "widow" is generally a later-in-life occurrence, women are more represented in the data than men. Whatever the case, it's clear being widowed sucks.
I expect to revise all these statistical risk numbers as I find more targeted or a accurate data.
Dr. Attia presents a slightly different statistical picture in the Early Medical program, organized around what he calls the "four horsemen of chronic disease." Unfortunately, the data sources aren't cited and I haven't been able to find them, so I have to trust his presentation, which is rigorous and thorough. Blending the data I could find with Dr. Attia's and my personal data (historical and empirical), I arrived at the following ranking for health risks:
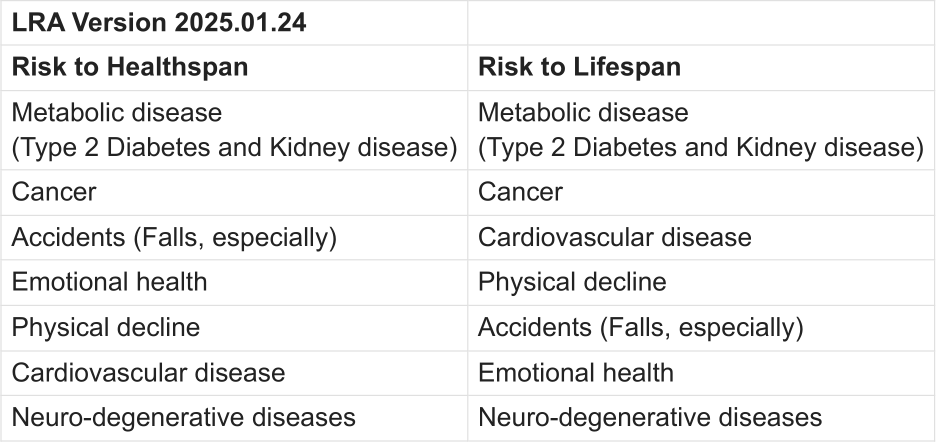
History and current blood markers are what put metabolic disease at the top of the list. It's the clear and present danger.
Even though I couldn't find a significant cancer history in my family, cancer occupies the second risk due to my age. Statistically, the longer we live the more likely we are to suffer a cancer diagnosis.
Early on in this exercise, I expected cancer would be high on my list because I live in Colorado. At 6,000 feet above sea level, the sun is much more intense. Except living in Colorado, it seems, continues to correlate with some sort of health benefit. Colorado has one of the lowest death rates due to cancer in the country. And according to the data for skin cancer, I needn't be as worried about this. Colorado ranks about mid-way for rates of skin cancer across all states (fully 1/2 that of Utah.)
I don't have a whole lot of confidence in this data, however. Many people in Colorado have moved here from other places in the last two decades and Colorado is known for one of the lowest obesity rates in the country. People here are health conscious and active. I think, however, there is a measure of transient resident bias in play here. Is it possible people live in Colorado during their healthy years but retire to somewhere else (usually warmer) where they eventually die? There is no data that I've found for cancer rates for people who have lived in Colorado all their life, like I have. I'm likely to be an outlier to the data and therefore consider my risk for skin cancer to be higher than what the data suggest. I've had several pre-cancerous skin issues over the years and so the plan is to continue seeing a dermatologist at least once a year, as I've done for the past 15 years.
Skin cancer isn't the only relevant age-related cancer risk. The rule-of-thumb wisdom in medicine is that most men die with prostate cancer, but only a few will die from prostate cancer. I already have issues with that pesky little gland and my PSA is one of the markers on the watch list. Again, Colorado ranks near the bottom for the rate of prostate cancer by state, but it's in the bottom of the top third for rate of death by prostate cancer. All this is tempered by the fact that with early detection the five year survival rate for prostate cancer is 99%. Left undetected until stage 4, the five year survival rate is less than 30%.
As I continue to age, accidents may take the number two spot. Particularly since I'm taking antihypertensive medications.1 I'm already out-sourcing various tasks, like clearing the rain gutters each fall and tree trimming, for which I no long feel physically capable of engaging without significant risk. As for dropping infectious diseases from the list, here's hoping no effing bureaucratic expert asshole is out there funding experimental gain-of-function virus research at Pangolin University.

Thus far in the Early Medical cartography effort, I have added the following to my marginal decade map:
A clear view of my marginal decade health goals
An assessment of the risks to my healthspan and lifespan
Family health history
Blood tests for 100 specific markers and a 10 year history for 50 of these markers
Several cancer screening tests
Heart calcium scan
Heart CTA scan
A closing thought on risks. They are not just statistical or actuarial. There is perhaps a larger set of risks buried within our beliefs, values, and biases. Perhaps they're outdated or uninformed or misinformed. Whatever the case, they are not serving us well and we probably aren't even aware of this fact. I've mentioned a few of my own - the reluctance to begin medication for blood pressure management and the ideas about health acquired during my early childhood.
There is one cognitive limitation that I think is particularly insidious: Denial. There are a whole host of cognitive biases and mental models that tangle together to form the denial Gordian Knot - confirmation bias, recency bias, optimism bias, cognitive dissonance, motivated reasoning - it's a big list. Cutting the denial Gordian Knot isn't easy. And throwing more knowledge at the problem usually isn't the answer. Smart people often have the tightest denial knots. The surgeon for my first wife's breast cancer, for example, the doctor that first alerted her to the problem, was later diagnosed with stage 4 breast cancer herself and died shortly thereafter. A highly skilled surgeon with the knowledge to diagnose an ailment in one of her patients neglected to diagnose the very same disease in her own body.
With a marginal decade/longevity risk assessment in hand, it's time to chase down the details. The next several posts will start to connect the historical and empirical dots of data, fine tune the risks, and start working on a strategy.
Disclaimer
The author is not a licensed practitioner of medicine or psychotherapy and nothing presented on this website claims or should be construed to provide medical or psychotherapeutic advice. This series of articles is presented as a personal reflection by the author on work he's done to improve his health and as such is relevant to the author and no one else. The author makes no recommendations as to any course of action the reader may chose to follow other than to encourage the reader to work closely with qualified health professionals when making healthcare decisions relevant to their personal lives.
← Health and Well-being - Part 6 - Empirical Data
"Health and Well-being - Part 7 - Assessing Risks" last updated on 2025.09.09.
Health and Well-being - Part 8 - The Critical Blocker →
I hope you will return regularly to The Remnant's Way as I often update posts, particularly Ab Initio, and do not always publish to email posts that are meant to support or serve as reference to existing or future posts.
And please consider becoming a paid subscriber. Doing so supports my writing efforts and grants me the most precious of all resources - dedicated time for writing. And for that, I am deeply grateful. If you prefer, buy me a cup of coffee if there is an article here and there that you enjoyed or found valuable.
Image credit: Grok 4
Footnotes
Attia, P., Alderman, J., & Birkenbach, K. (2024, December 12). A link between antihypertensive medications and fall risk reminds us to take precautions. Peter Attia, MD. https://peterattiamd.com/fall-risk-and-antihypertensive-drugs/